Achilles Tendon Problems
What is it and how can we help it?
Dr Jed Pullen – Senior Osteopath & Marathon Runner
What is it?
The achilles’ tendon is the lower attachment of the calf muscle onto the ankle. Achilles’ tendon issues often occur due to an increase in load through the lower limb and calf muscle. Overloading the tendon can result in tendon related problems. Increasing age, being male, and obesity can also increase your likelihood of injury.
Why do Achilles Tendon Problems occur?
2 theories exists:
1) Chronic degeneration: Chronic degeneration of the tendon may lead to a rupture without the need for excessive loads to be applied. It is also thought that impaired blood flow to the tendon with resultant lack of oxygen and altered metabolism could play a major role in injury.
2) Mechanicaltheory: Movement and force applied to the tendon may lead to tendon failure. Push off activities where the muscle and tendon has to go from a shortened position to near maximal contraction are likely culprits..The risk of injury increases when the body is unable to reduce excessive and uncoordinated muscle contractions. This is often seeing in those who train less such as the weekend warrior.
Types of Achilles Tendon Problems:
1) Chronic Achilles Tendinopathy
2) Achilles’ Tendon Rupture
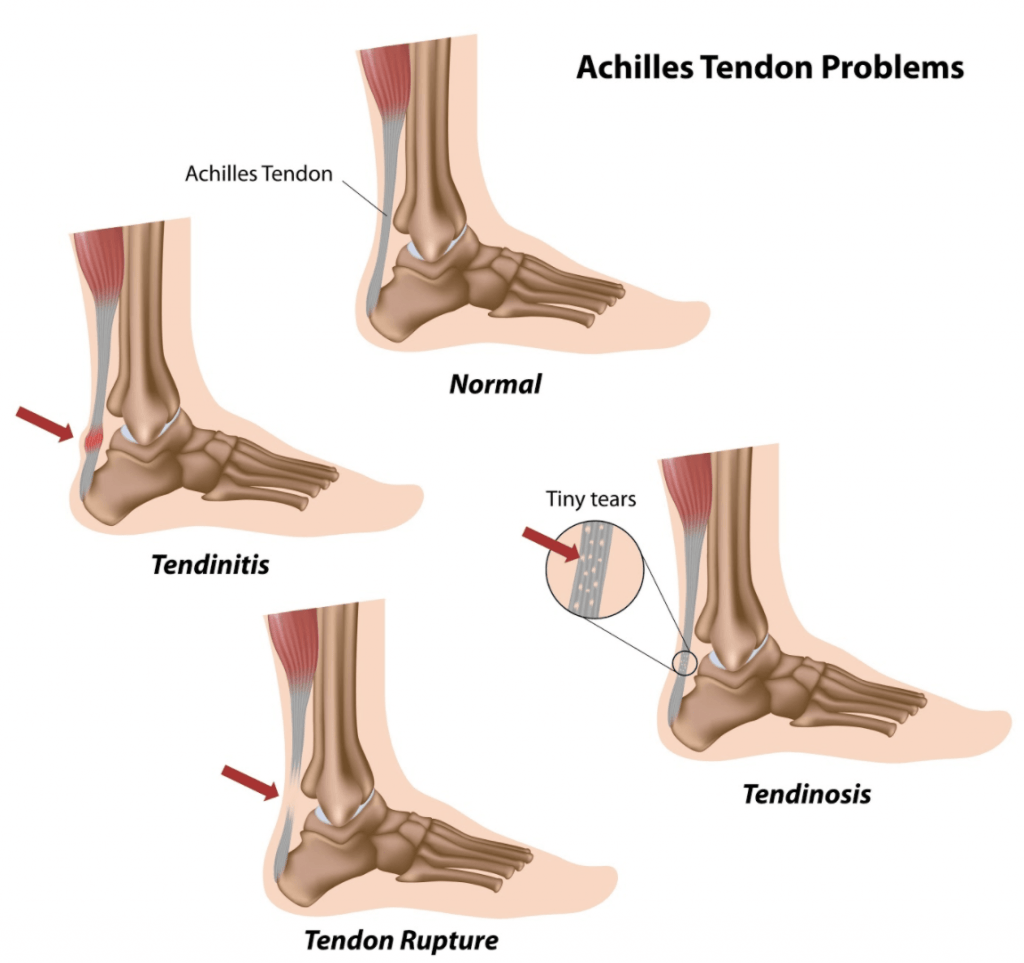
1)Chronic Achilles Tendinopathy
Typically found in middle aged, male runners and is also associated with overuse/excessive load. It has been found that there is a 10 x increase in injuries in those that run compared to non-runners at the same age. 31% of those injured did not do vigorous activity which points to the fact the cause may be related to other influences. Metabolic or circulatory imbalances may be culprits. When we look at the tendon under a microscope we often find a change in structure without inflammation. This changes in collagen structure shows us that this is primarily degenerative yet non-inflammatory problem.
We find this in 2 places. 55-65% of the time it is located in the middle of the tendon and 20-25% it will also lie at the insertion of the achilles.
1a) Non – Insertional Achilles Tendinopathy
Pain: Beginning and shortly after finishing exercise.
Location: Most of the time it is located 2-6 cm above the attachment onto the heel.
Management:
- Modifying activities, eccentric exercises, anti-inflammatories, injection and Shockwave therapy.
- Eccentric heel drops: At 12 weeks 36/41 had no further tendon pain and the structure of the tendon had normalised.
- Injections: These may be used to provide pain relief but must be completed under ultrasound. It is important to note thought there is a possible risk of future rupture due to the effect of corticosteroids. Platelet-rich Plasma is another option also a possible injection and has shown inconsistent results.
- Surgery: This can also be an option if conservative treatment fails.
1b) Insertional Achilles Tendinopathy
Degeneration of Achilles’ tendon fibres at the insertion of the Achilles. This is normally associate with older age, steroid use, obesity, diabetes, and inflammatory conditions.
Pain: Mid point of the Achilles, worse in the morning and also very sore day post exercise. These individuals may also have prominent boney prominence near the top of the heel.
Management:
- Activity modification is key: Reduce walking up hill, shoe lifts will help avoid pressure.
- Eccentrics strengthening : Typically make this worse due to compression of the tendon.
RUNNERS + ATHLETES: How can we keep on moving and exercising whilst managing an Achilles’ tendon problem?
The last thing a runner wants to hear is to stop running all together. We need to manage the load going through the tendon to allow healing and reduce aggravation. One of the first questions we should ask ourselves is, “What has changed?”. Something has changed a sudden increase in load, a sudden increase in speed, a sudden increase in hills, a sudden increase in kilometres, a sudden change in gym work out, shoes, surface etc. A sudden change normally precipitates an injury.
We can massage the area to desensitise it, we can use rock tape which may provide the body with additional feedback and we can strengthen it. If we don’t take some load off the area then we won’t allow healing. How do we do this?
- Reduce Intensity: Slow down your runs to a pace where your body is able to absorb the load.
- Avoid running up hills: This stresses the back of the leg. It is great when you are healthy to strengthen the calf but can put undue stress on the achilles.
- Running technique: Improving your running technique can be very helpful to avoid undue pressure going through your body. You may need to revert back to your old technique because you suddenly changed your style.
How do you know if you have done to much and overloaded the tendon?
There are 3 parameters that I look at for: .
1.Pain during your work out
2. Pain for more than an hour after your workout
3. Pain the next morning/day
The most overlooked parameter is pain the next day. People often don’t know what has flared them up as they felt great during their workout. Keep a look out for this key sign.
2) Achilles Tendon Rupture
It is common for ruptures to occur in healthy, active, young to middle age people approx 37 -43.5 years of age, with a ratio of M/F 5:1.
The tendon most commonly ruptures through the mid section 3- 6 cm from the achilles attachment often where there had been no prior pain. A sharp forceful push off or abrupt activity often causes it to rupture.
Alternatively you can get a tendon rupture where it attaches onto the bone. Normally this happens after ongoing pain for a period of time.
Should i get a scan on a rupture?
Scans aren’t completely necessary as this can often be diagnosed clinically by assessing the area. If we think surgery may be an option a scan is usually ordered to asses the severity of the tear. Surgery may be indicated if a gap of more than 5mm is found. Surgery can reduce the risk of tearing it again by 8.8% but comes with other complications.
Take Home Message!
Overall Achilles Tendon Problems can be a frustrating. The journey to full recovery is often a marathon not a sprint. Exercise and load management is the key to proper recovery of these particular injuries. Maintaining some form of load is also important, with the exception of tendon ruptures, to ensure the muscle is maintaining strength. 12 months of an evidence based loading program must be included for full recovery. It has been found to better than surgery to reduce pain and function. Seeking help from your qualified health professional as to the proper management regime is very important.
Load management, load management, load management is the a key to prevention and recovery of this often cranky ongoing tissue injury.

Written by:
Dr Jed Pullen – Senior Osteopath. Move Osteopathy. Marathon Runner
Dr Jed is available Monday to Friday at our Brisbane CBD Clinic. Book Online Here